
Infobiogen : portail santé et bien-être
Découvrez tous nos articles pour rester en bonne santé ! Il n'a jamais été aussi important de rester en bonne santé vu l'effet positif sur presque tous les aspects de notre vie. Rester en forme peut se faire de différentes méthodes, notamment en mangeant des viandes maigres et saines et en consommant beaucoup de fruits et de légumes. Passer un peu de temps chaque jour à faire de l'exercice peut nous aider à être en bonne santé et à éviter les problèmes de santé.
Les opportunités de la franchise diététique en France

En France, le domaine de la diététique connait une croissance grandissante, et une forte demande en ce qui concerne les solutions nutritionnelles à adapter aux besoins individuels des consommateurs. Ces derniers, qui prennent de plus en plus conscience de l’importance … Lire plus
Comment trouver le caviste idéal pour du vin bio ?

Lorsque l’on est passionné de vins, le choix d’un caviste est très important. Il est parfois difficile d’accorder sa confiance, mais certains critères permettent de trouver la cave à vin idéale, et ainsi de profiter de vins bios de qualité, … Lire plus
Prévention des troubles musculosquelettiques : le rôle du siège ergonomique

Touchant les membres supérieurs et le dos, les troubles musculosquelettiques (TMS) peuvent apparaitre ou être aggravés à cause de l’activité professionnelle. Réduire les contraintes et aménager les postes de travail avec un siège ergonomique professionnel peuvent néanmoins permettre de les … Lire plus
Les avantages de la permanence téléphonique médicale pour les patients

La permanence téléphonique médicale offre de nombreux avantages aux patients, en leur fournissant une assistance médicale accessible et pratique en dehors des heures d’ouverture des cabinets médicaux. Ces avantages contribuent à améliorer l’accès aux soins et à renforcer le soutien … Lire plus
Comment les informations médicales sont-elles traitées dans le cadre du télésecrétariat médical ?

Dans le domaine du télésecrétariat médical, le traitement des informations médicales revêt une importance capitale. Les télésecrétaires sont responsables de la gestion, de la sécurité et de la confidentialité des données médicales des patients. Découvrez comment les informations médicales sont … Lire plus
Quels sont les avantages et les bienfaits d’un pistolet de massage musculaire ?

Le pistolet de massage musculaire est devenu un outil de plus en plus populaire pour la récupération musculaire et la détente. Grâce à ses vibrations puissantes et à son action ciblée, il offre de nombreux avantages et bienfaits pour le … Lire plus
Quels sont les bienfaits du massage musculaire sur le corps et la santé ?

Le massage musculaire est bien plus qu’un simple moment de détente. En plus de procurer une sensation de relaxation profonde, il offre de nombreux bienfaits pour le corps et la santé. Que ce soit pour soulager les tensions musculaires, améliorer … Lire plus
La formation SST : un investissement pour la santé de tous
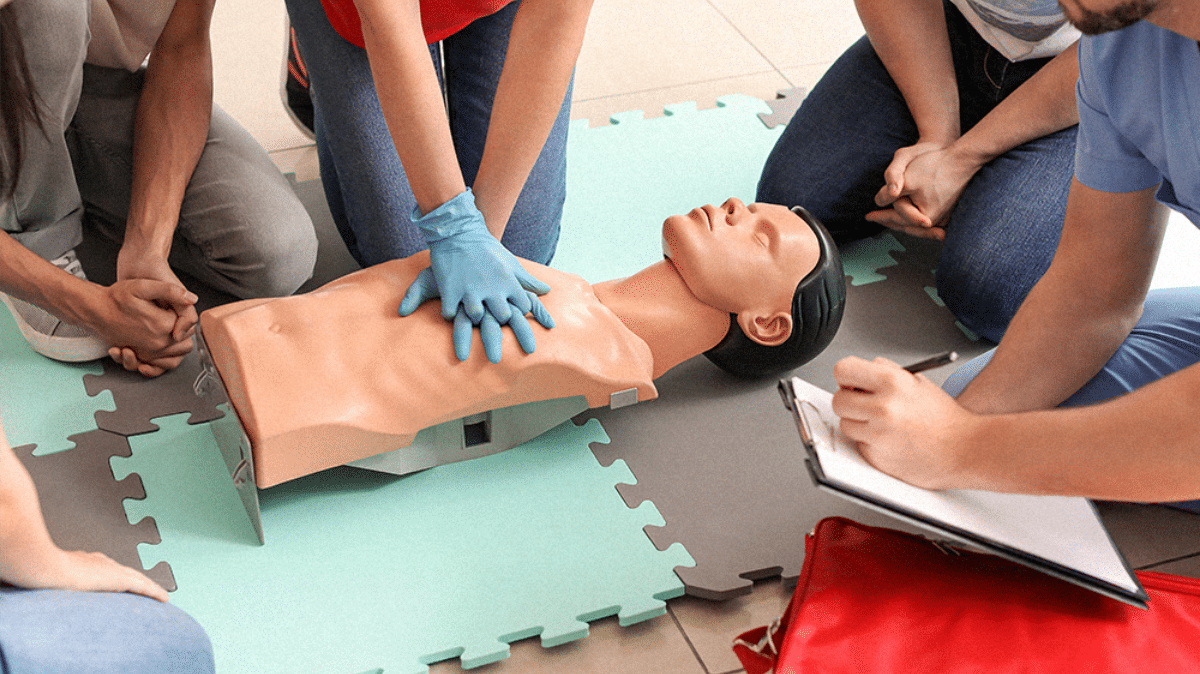
Pour chaque entreprise, la sécurité est un point indispensable, et ce peu importe son secteur d’activité, sa taille, ou le nombre de ses salariés. Il s’agit d’une responsabilité, et même d’un devoir, des chefs d’entreprise afin d’assurer la sécurité et … Lire plus
Quels sont les avantages et les inconvénients de l’épilation définitive ?

L’épilation définitive est une option populaire pour les personnes souhaitant se débarrasser des poils indésirables de manière permanente. Cependant, comme toute intervention esthétique, il y a des avantages et des inconvénients à prendre en compte avant de choisir cette méthode … Lire plus
Quelles sont les interventions les plus courantes en chirurgie esthétique ?
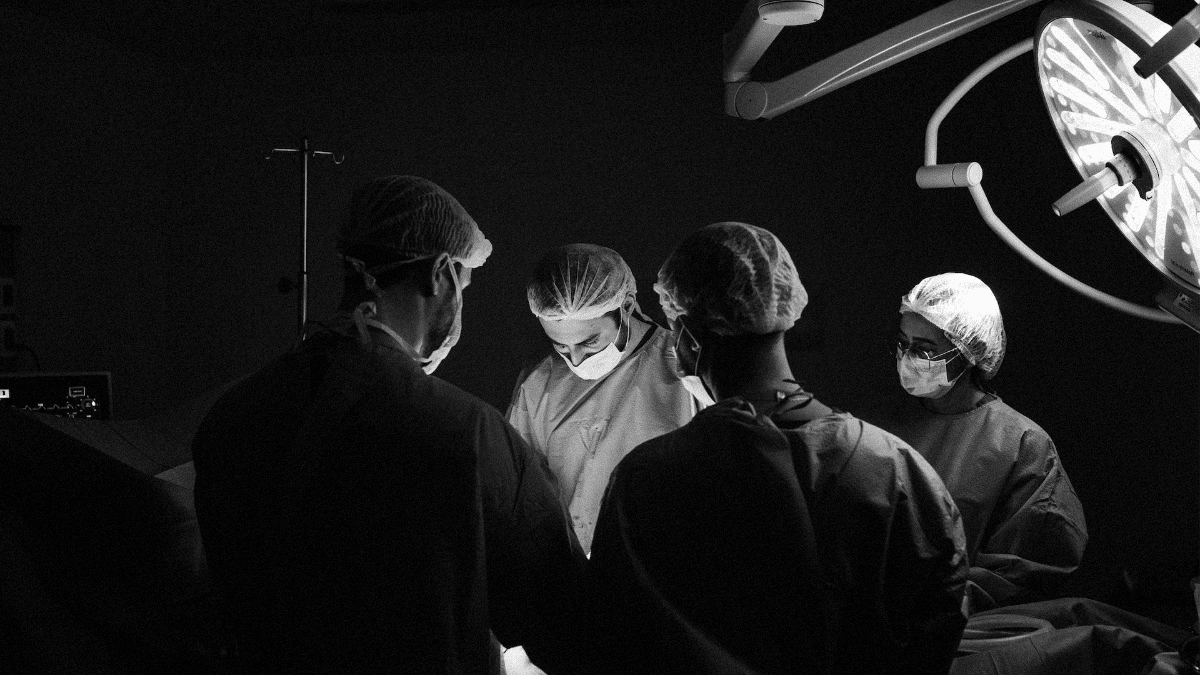
La chirurgie esthétique est de plus en plus populaire dans le monde entier. Les interventions les plus courantes sont souvent choisies pour améliorer l’apparence physique et aider les gens à retrouver leur confiance en soi. Dans cet article, nous allons … Lire plus
Quels sont les avantages de l’allaitement pour le bébé et pour la mère ?

L’allaitement est un choix personnel pour chaque mère, mais il est important de comprendre les avantages pour le bébé et pour la mère. Non seulement l’allaitement fournit une nutrition optimale pour le bébé, mais il peut également renforcer le lien … Lire plus